
Blog

Art and Science I: Please hold the Science
When I bring up the research from clinical psychology on outcomes of psychotherapy, other therapists say to me, “Psychotherapy is an art and a science.” Yet I’ve had one colleague say to me, “Science can’t tell us anything since it’s always changing its mind.” Another told me, “Science cannot reveal anything about therapy because therapy is about human relationships...”
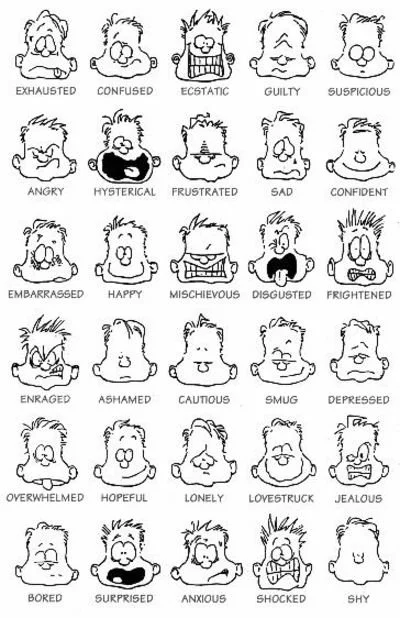
Anxiety Part One: “What It’s Like”
Emotions are tricky - they’re like colors. Understanding facts about colors doesn’t seem to give us all the information...
Recommended by AstralCodexTen SlateStarCodex Psychiat-List
Scott Alexander is a psychiatrist on the West Coast who blogs about science, medicine, philosophy, politics, and futurism. His blog is one I’ve followed for a few years now, and I find it to be one of the best sources for dispassionate and well-informed takes on difficult subjects which do not admit to easy answers. His writing demonstrates how to approach questions in a way that improves the accuracy of our beliefs and the application of our values...
Frequently Asked Questions About Drugs and Addiction
Is it normal to use drugs? We see the drive to alter consciousness across time and cultures. Every culture has norms and rituals for preparing and using psychoactive substances. As a Human Universal, it’s hard to say that altering consciousness is not normal behavior...
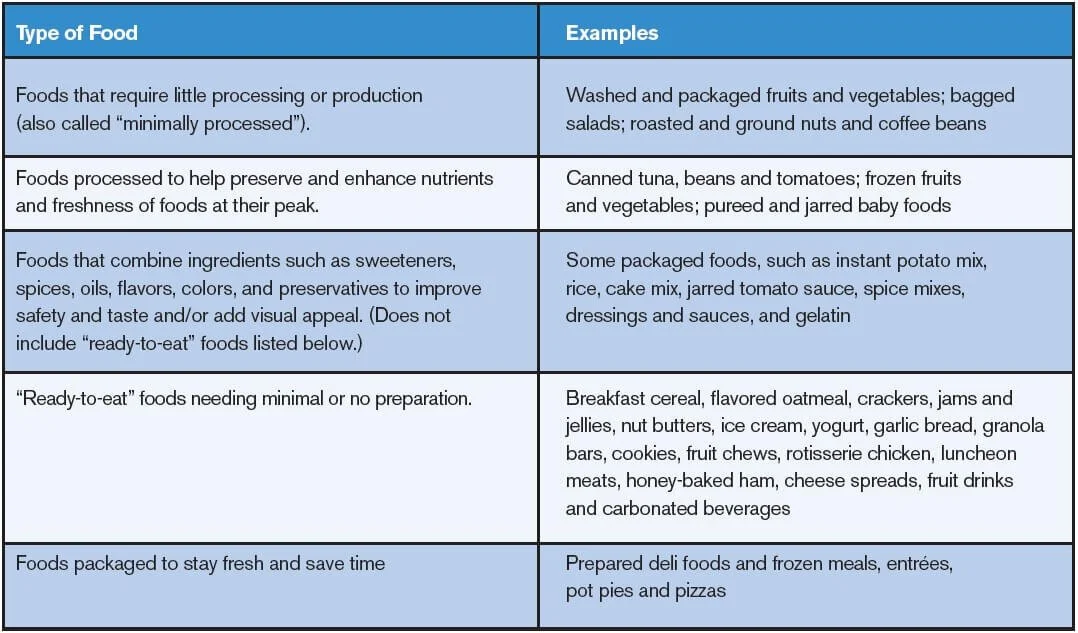
Evidence Based Wellness Choices to Make Life Better
To best understand the role of diet, exercise, and sleep, begin with a detailed journal. Using an app like MyFitnessPal is a quick way to start a food journal. Documenting is an excellent way to learn calorie and nutrition content and gain insight regarding what your choices really entail...