Art and Science II: The Great Psychotherapy Debate
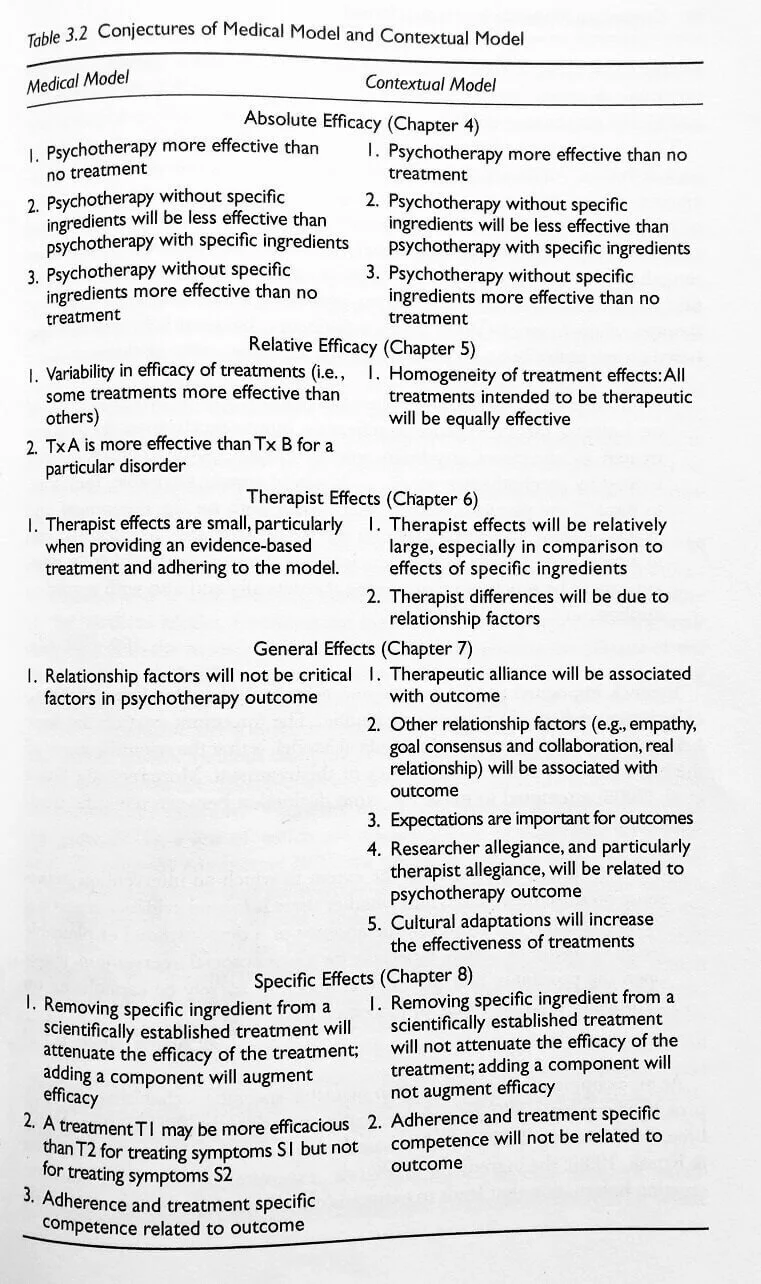
For the better part of a year, I have been reading Bruce Wampold’s book, The Great Psychotherapy Debate. It’s a white paper examining the evidence for two competing models of interpreting the research on outcomes in psychotherapy. The competing models for interpreting the research are The Medical Model and The Contextual Model...

Art and Science I: Please hold the Science
When I bring up the research from clinical psychology on outcomes of psychotherapy, other therapists say to me, “Psychotherapy is an art and a science.” Yet I’ve had one colleague say to me, “Science can’t tell us anything since it’s always changing its mind.” Another told me, “Science cannot reveal anything about therapy because therapy is about human relationships...”