
Blog

Erotic Intelligence: How to Cultivate Healthy Sexuality in Intimate Relationships
Erotic intelligence is a concept created by Esther Perel, a Belgian-born psychotherapist, author of the best-selling book Mating in Captivity: Unlocking Erotic Intelligence. This book discusses the conflict between sex and intimacy that afflicts many modern couples. It’s worth spending time to examine the key concepts of Erotic Intelligence and how to apply them to cultivate healthy sexuality in intimate relationships.
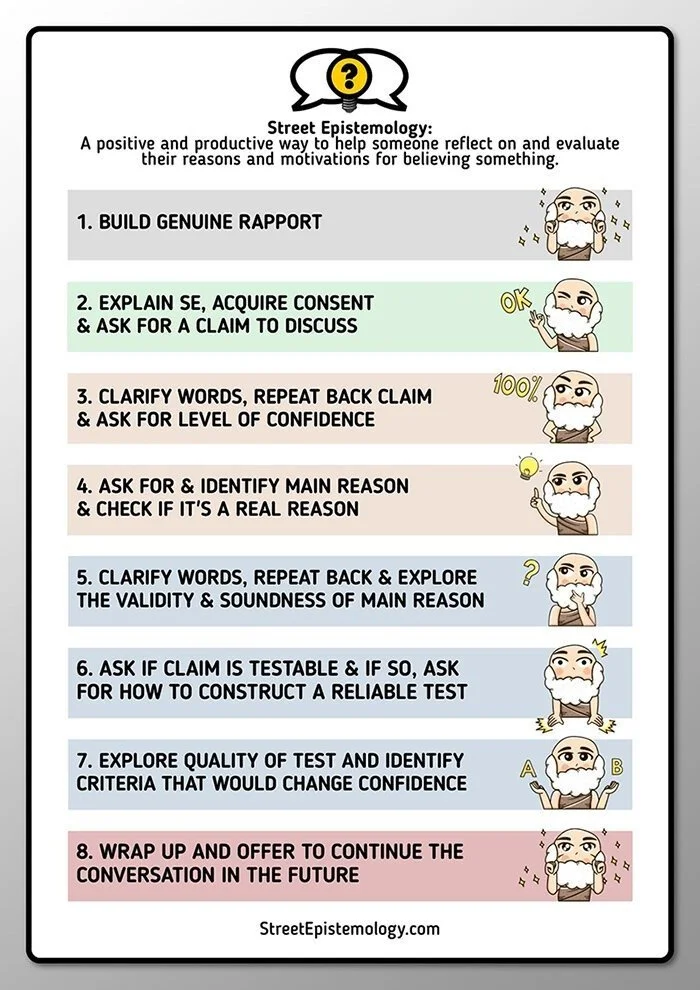
Interview with Reid Nicewonder, the Cordially Curious Street Epistemologist
There’s a contradiction that sometimes occurs when someone comes into therapy. A client will sit down and express certainty about their inadequacy, badness, and helplessness yet they are entering a space expecting to change. They experience the ambivalence between feeling the belief in their badness, inadequacy, and helplessness is true and expecting that it can be shown to be not true.
Anxiety Part Two: Anxious Like Me
To the best of my understanding, theories of emotion are attempts to answer the question, “WHAT IS THIS FEELING, WHY DO I HAVE IT, AND WHAT’S WITH THIS SALTY DISCHARGE COMING FROM MY EYES?” Thankfully, we’ve mostly outgrown humour theory, so relatively few people still say you’re depressed due to an excess of black bile. But then again, within the last month, I heard people attribute feeling states to another ancient theory of medicine...
Art and Science III: SlateStarCodex on Gottman
Scott Alexander, my favorite writer on the interweb, has been reviewing therapy books and got around to a particular specialty of mine, couples therapy. He reviews John Gottman’s landmark book, Seven Principles for Making Marriage Work...
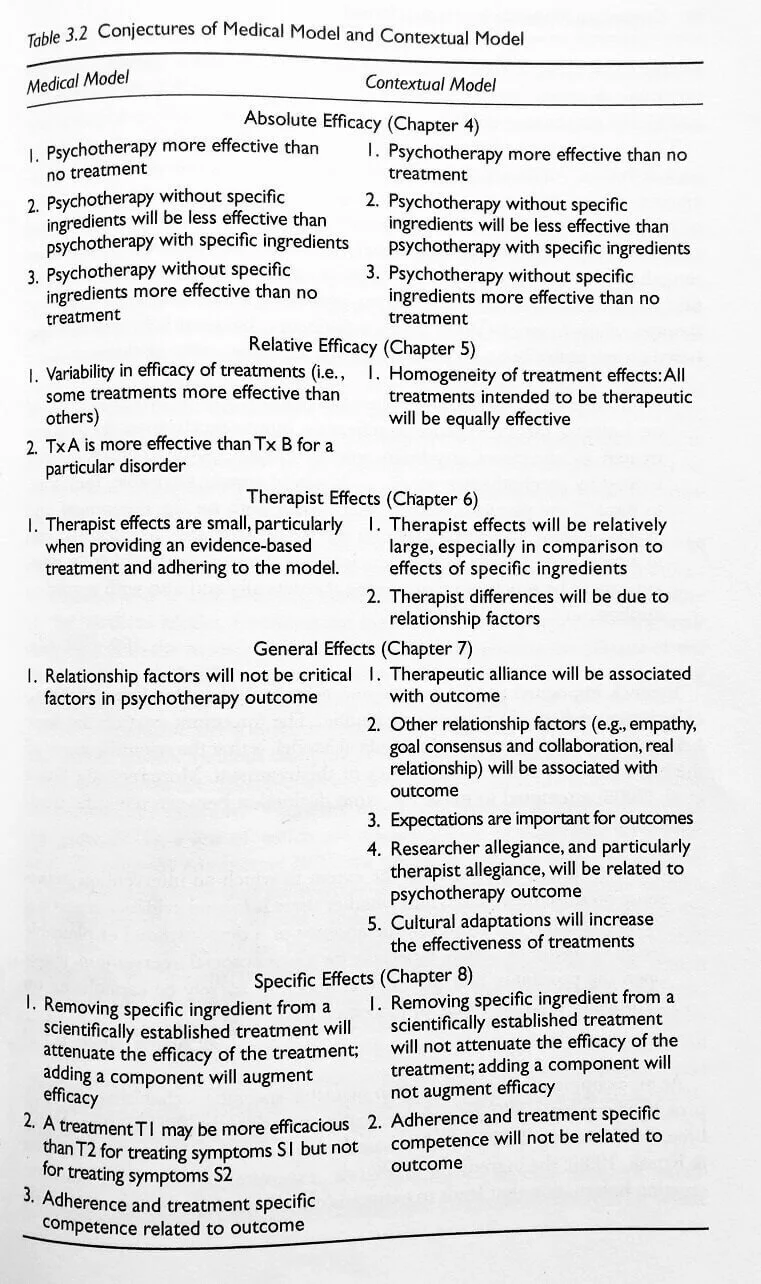
Art and Science II: The Great Psychotherapy Debate
For the better part of a year, I have been reading Bruce Wampold’s book, The Great Psychotherapy Debate. It’s a white paper examining the evidence for two competing models of interpreting the research on outcomes in psychotherapy. The competing models for interpreting the research are The Medical Model and The Contextual Model...